INTRODUCTION
Second-hand smoke (SHS) exposure is a serious cause of ill health for children, contributing to illnesses such as meningitis, respiratory infections and sudden infant death syndrome. Worldwide, it is estimated that more than 40% of children are regularly exposed to second-hand smoke in the home1. Second-hand smoke can persist indoors at potentially harmful levels for long periods following even one cigarette2. Reducing this exposure is a public health challenge that has been embraced by policymakers and regulators3,4. However, there are few interventions that are effective in reducing SHS in deprived households with children5.
Fine particulate matter (PM2.5) is a significant component of indoor air pollution, and has been widely used in tobacco control research as a marker for the presence of SHS6. Indoor air quality monitoring and feedback therefore has been explored as a potential motivator in interventions to encourage parents to keep smoke-free homes7–9. However, there is currently little evidence of interventions that have solid theoretical foundations in behaviour-change theory.
AFRESH (Finding Ways to Reduce Second-hand Smoke Exposure in Homes), a novel intervention to promote smoke-free homes, was developed using intervention mapping10 to systematically develop a theory- and evidence-based behavioural intervention to reduce second-hand smoke in deprived households with children, with air quality feedback as a central component of the behavioural strategy. The full description of the intervention and its development process will be published separately.
The aim of this study was to evaluate the feasibility and acceptability of delivering this theory-based intervention through small third-sector organisations in deprived areas within Scotland. While previous research in this area has relied on researchers providing air quality information to participants7, the present study gave full responsibility to non-technical staff, thus testing the feasibility of the intervention in a real-world setting.
METHODS
AFRESH intervention
The AFRESH intervention is designed around the delivery of personalised air quality information to parents who do not live in smoke-free homes in deprived settings. The intervention is designed to be delivered by support workers employed by third-sector organisations, therefore widening the potential group of people who can deliver it by researchers and healthcare workers, as used in previous research7. The intervention is designed to be simple to deliver, to use a low-cost monitor and is structured around a series of modules and contacts between the worker and the parent: full details are available in the supplementary material11.
For this feasibility study, third-sector community centres were invited to take part, with their support workers receiving training on the intervention from the research team. Parents with a child under the age of six living in a smoking home were invited to participate in the intervention by a support worker. Following informed consent, the participant was given information about SHS by the third-party worker and provided with an air quality monitor to place in the home for approximately five days. Following the measurement period, the monitor was returned to the worker who then prepared an air quality report. Custom software12 developed for AFRESH was used to facilitate the support worker in downloading and processing data, and in the preparation of air quality reports.
The report was given to the participant, and used as a focus to discuss planning for a smoke-free home with the worker. These discussions included techniques to allow exchange about the issue of SHS with other smokers and the available support to quit smoking entirely.
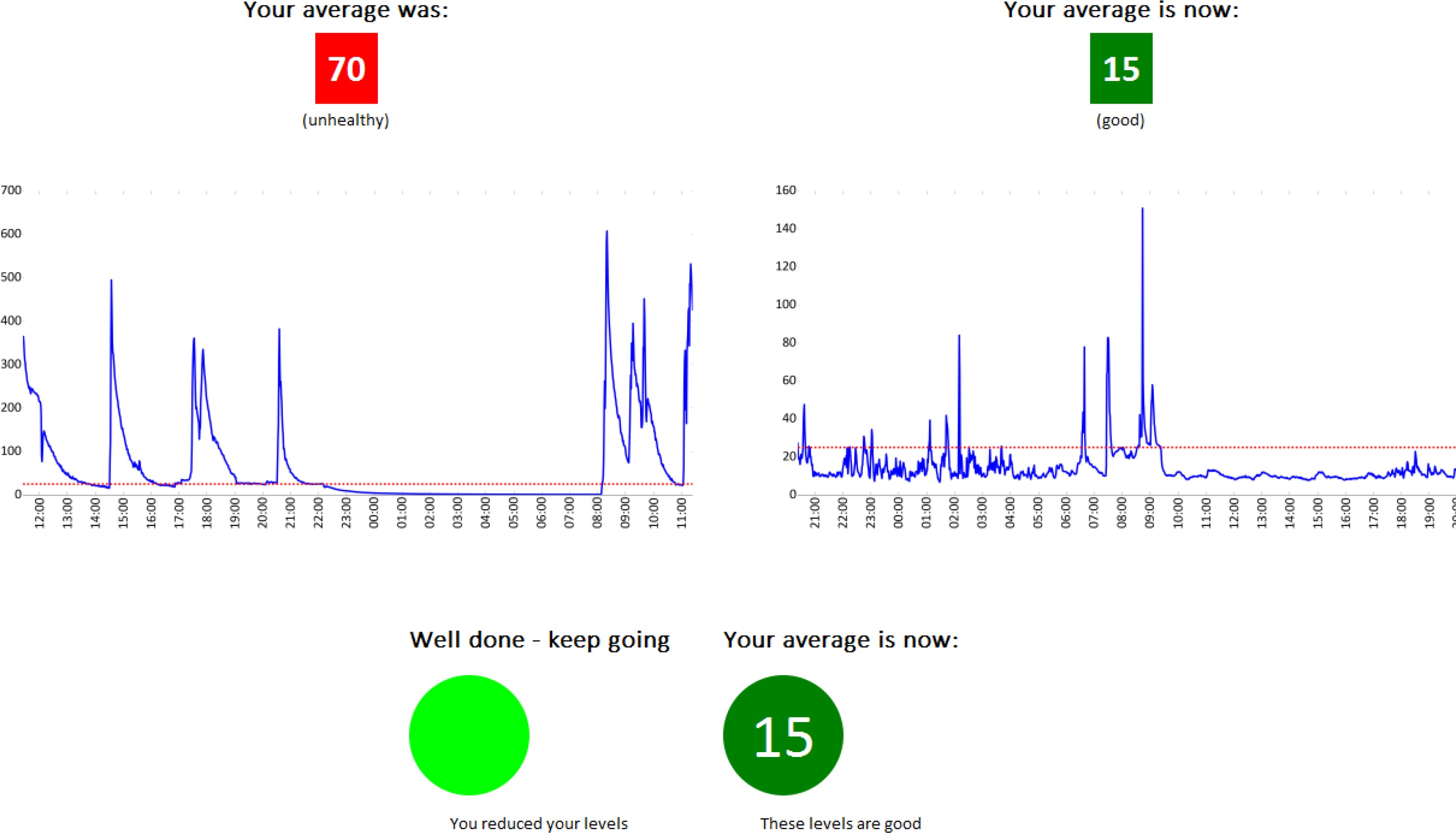
Two weeks later, the monitor was returned to the participant’s home for another five-day period. A second report was produced including a comparison sheet (Figure 1). The worker and participant then discussed successes and challenges in keeping a smoke-free home.
Ethics
Ethical approval was provided by the College Ethics Review Board, College of Medicine and Life Sciences, University of Aberdeen.
Recruitment
A target of 20 intervention participants between two third-sector centres was set at the beginning of the study, which was believed to be attainable based on previous work in this setting and in-line with the literature on good practice for feasibility studies testing intervention efficacy13.
Community centres were approached to take part through pre-existing relationships with research staff. These third-sector organisations employed workers in direct contact with members of the target population.
Training
Support workers taking part in the intervention were trained over two to three hour sessions. The first gave information about SHS and its effects on health and air quality, while the second gave information about the intervention. Following this session, an online course was developed to allow others to use the intervention14.
Analysis
The primary outcome measure for intervention efficacy was the change in average PM2.5 measured in each home following the intervention. Secondary outcome measures included self-reported changes in the rules of smoke-free home, including participant and staff experiences in using the intervention.
Qualitative interviews
Up to 10 parents were to be invited to take part in an individual telephone interview at the end of the intervention to explore; their experiences in taking part, and the impacts of the feedback they received on their smoking behaviour in the home. Support workers were also invited to take part in interviews at the end of the intervention, to explore their experiences during intervention delivery. These interviews used a semi-structured format.
RESULTS
Recruitment
One of the six centres invited to take part agreed to participate. In this centre, four participants were recruited and three of these participated in qualitative interviews. Five centres declined to take part citing reasons such as: staff turnover (n=1), lack of staff time (n=2), inability to recruit sufficient members of the target population (n=2), and the perceived intrusiveness of the intervention (n=1). One centre gave multiple reasons for declining to participate.
Quantitative results
Household average PM2.5 levels were lower in all four homes following the intervention, but the small sample size precluded statistical significance.
Baseline measurements lasted for durations between [5 days, 26 minutes] and [6 days, 6 hours, 22 minutes], while follow-up data were measured for durations between [3 days, 23 hours, 53 minutes] and [5 days, 7 hours, 15 minutes]. While the programme material suggested carrying out follow-up measurements two weeks after the end of the baseline measurement, in practice follow-up measurements began 18-39 days later (mean 28 days).
The mean measured PM2.5 was 80.5 μg/m3 (range 11-239 μg/m3) at baseline and 66 μg/m3 (range 6-201 μg/m3) at follow-up. Reductions in average PM2.5 over this period ranged from 2-38 μg/m3, but no home that had an average PM2.5 measured above the WHO guidance level at baseline had an average concentration below this value at follow-up.
Parent perceptions of the intervention
Three of the four participants consented to take part in a semi-structured telephone interview, conducted by a member of the research team, to discuss their experience of the intervention.
Changes to smoking behaviour were noted by two participants as a result of their personalised feedback; one had started smoking outside instead of indoors; a second was smoking inside, but now with the window open. The third had moved home between measurements, and was now smoking outside as smoking inside her new flat was prohibited as part of the rental agreement.
Parents stated that the intervention was acceptable, and found the air quality feedback reports understandable and meaningful:
“The graphs were quite understandable. It showed me the peak times [when SHS was highest]. It was very accurate too – I could see when I was smoking in the home and it was right”
When asked about benefits of taking part, all three commented on knowledge they had acquired through participating, for example:
“I’ve noticed that it [SHS] does linger longer than I thought it did. So when I come down in the morning, it’s all clear [the air], but the machine says not.”
“Now I know that it can make a difference to your kids if you don’t smoke in the home. It’s basically not normal to smoke around your children.”
“I’ve learnt that second-hand smoke is more harmful to kids than it is to adults. And that second hand smoke can cause asthma in children – I thought you were just born with it.”
Worker perceptions of the intervention
The support workers were also interviewed about their experience of delivering the intervention. They valued the training received prior to conducting the intervention, and highlighted the importance of existing relationships with parents to aid recruitment. They spoke of capacity issues limiting recruitment given they were the sole worker on the project within their organization:
However, the staff member felt that the intervention itself was feasible and that feedback reports had the potential to change smoking behavior in the home, “especially with those that were high levels, because you could see that they were quite shocked with it, and it was interesting, just that graph and all the different colours and stuff. The colours really helped actually.”
They considered that the intervention would be
DISCUSSION
Recruitment of centres
The main finding from this study was that recruiting centres to take part was problematic. The multi-step nature of the intervention was perceived to be excessive for reasons that included too great an impact on staff time. Carrying out one intervention requires five to seven contacts between a worker and a participant. This can involve travel to the participant’s home or another location that potentially can take more time.
Even centres that initially expressed eagerness to take part were sometimes unable to do so, reflecting the high workload, limited resources and short-term funding cycles of the third-sector organisations approached. Expense could be another factor constraining the use of the intervention. The cost of purchasing the relatively inexpensive Dylos DC1700 can exceed £400 GBP (500 USD), a substantial sum for a small organisation. Staff time would represent an additional cost - assuming an hour per contact paid at the median UK hourly wage (£11.78 in 2015)15, this would range from £58.90 - £82.46 per intervention. These costs would not apply where air quality monitoring equipment was already available, or in countries where labour costs are substantially lower than in Scotland.
The perceived inability to recruit smoking parents was unexpected since our previous experience was that many clients who were invited to take part and who attended the centres were regular smokers. Better-funded statutory bodies or recruiting participants directly may ameliorate these issues. The challenge in recruiting community “champions” is an important message for future studies and suggests that specific staff dedicated to smoke-free homes interventions are required rather than seeing this as an ‘add-on’ to the already high workload of support staff or support workers dealing with parents in deprived settings. Contacting potential partner organisations further in advance than the timeline of this study permitted, or providing them with financial compensation for engaging in the intervention programme, may improve participation rates.
Feasibility of the intervention
This feasibility study demonstrated that while the AFRESH intervention could be delivered by third-sector organisations working with individuals in low socioeconomic groups, the difficulties in doing so are substantial. Participants could understand, interpret and accept the results of air quality monitoring and, as with previous studies7, this may assist in encouraging changes to smoking behaviours.
All participants experienced reductions in household average PM2.5 concentrations by follow-up measurements though some changes were small. Carrying out the follow-up stage of the intervention repeatedly over a longer period may motivate participants to continue making changes, and provide evidence of the effectiveness of the different elements within the AFRESH programme.
CONCLUSIONS
Overall, those participants and workers who took part found the AFRESH programme acceptable and useful, but difficulties recruiting centres to take part would make the programme impossible to use widely in its current form. SHS levels fell modestly in all four homes, although the small sample size made statistical analysis of this decline impossible. Working with small community-based third-sector organisations presents practical and logistical challenges and these would be a significant barrier to using this model widely to promote smoke-free homes. Future research should focus on efforts to reduce the time and number of home visits or face-to-face contacts required to deliver the programme to those who express interest.