INTRODUCTION
Drugs are a variety of substances, both natural and chemical compounds, that are classified as narcotic substances due to their high potential for dependence. Drug consumption is increasing and reports suggest that about 2 billion people consume alcohol, 1 billion smoke tobacco, and 270 million use other substances continuously, worldwide1. Meanwhile, drug use in young people, especially among students, has increased. In research conducted among governmental universities in the Tehran province in the 2001–02 academic year, the rate of cannabis and opium use were reported to be 0.2% and 0.3%, respectively2, while these figures increased to 0.6% and 0.4% in 2005–063. In another study conducted in 2010, the rates of cigarette smoking and hookah consumption among students of governmental universities were 30.8% and 40.3%, respectively4.
The high prevalence of drug use among students has raised concerns about their health. Numerous reports suggest that cigarette and tobacco smoking among juveniles results in many diseases such as cardiovascular and metabolic diseases, cancer, pulmonary disease, problems in pregnancy, as well as premature death5. So considering this issue and applying strategies to reduce drug use among students, is a prerequisite to improving the health of the community. On the other hand, dormitory students face many challenges, due to passing through high school and starting to live in dormitories, such as new roommates, changes in living patterns, problems with planning, and a need to become more independent, all of which contribute to stress and are usually associated with sleep disorders and low level quality of life. Previous studies have shown that about 73% of dormitory students have experienced low sleep quality6. Also decreased sleep quality is associated with cardiovascular diseases, metabolic syndrome, obesity, and hypertension7.
Identifying and controlling the factors that affect quality of life and sleep quality is important to improving the health, well-being and academic achievement of students. Therefore, evaluating health-related indicators such as addiction, quality of life and sleep can provide valuable information to improve health and prevent dangerous behaviours. One of the most cost-effective and immediate ways to evaluate quality of life, sleep and drug use is to use questionnaires such as ASSIST, PSQI and SF-36. These questionnaires have been translated and validated into many languages and are being used in several countries as well as in Iran8,9. Many studies have shown a relationship between drug use, poor quality of life and sleep with a variety of non-communicable diseases such as cardiovascular diseases, metabolic diseases, and mental diseases including depression, anxiety, and stress10-12. Many studies have shown a negative relationship between drug use and sleep quality and quality of life in different individuals13,14. According to the National Institute on Drug Abuse (NIDA), many sleep disorders are caused by the use of various drugs and addictive substances14.
Despite the prevalence of drug use, particularly among students, there has been little research on the effects of these substances on the sleep quality and quality of life in dormitory students. Also, most studies in this area are conducted on one or two drugs, and it is clear that there is insufficient research on the use many types of drugs among students. Therefore, the purpose of this study was to investigate the relationship between drug consumption and sleep quality and quality of life in dormitory students of Allameh Tabataba’i University, Iran.
METHODS
Subjects
This descriptive study was conducted with the use of a questionnaire. A sample size of 324 out of 2100 students who live in the Allameh Tabataba’i University dormitories was selected using Cochran's formula with a 95% confidence interval and 5% error. Students were randomly selected from all grades and disciplines, comprising 420 students with 240 females and 180 males.
A detailed explanation of the research aims was presented to the students and the subjects completed consent forms. The inclusion criteria included: having an Allameh Tabataba’i University student card and living at least three months in dormitories. The exclusion criteria included: age over 40 years (because of the small number of subjects aged >40 years and also for data normalization) and being on the menstrual cycle (due to its negative effects on sleep quality)15. Twenty subjects were excluded because of incomplete questionnaires, 8 females who were on the menstrual cycle, and 2 others for being outside the included age group. Finally, 392 students (222 females and 170 males) were included in the study.
Questionnaires
Drug use assessment
The ASSIST questionnaire was used to assess drug use. The questionnaire consists of 8 sections and evaluates the use of 10 different types of drugs: tobacco, alcohol, cannabis, cocaine, amphetamine-type stimulants, inhalants, sedatives, hallucinogens, opioids, and other drugs. In addition, it provides information on the narcotics that people have consumed over their lifetime, the substances that have been used in the past three months, problems related to substance use, risk of current or future harm, drug dependency, and injecting-drug use. The scoring of this questionnaire is in the form of a Likert scale with a score above 27 for each drug representing a high risk. The reliability of each of these ten substances ranged from 0.61 to 0.78, which is an acceptable coefficient. Also, the validity of the questionnaire was 0.8416.
Sleep quality assessment
The Pittsburgh 19-item questionnaire (PSQI) was used to evaluate the students’ sleep quality. The scoring of this questionnaire is in the form of a 3-point Likert scale. The summing of seven component scores calculates the global PSQI score. A global sum ≥5 indicates poor sleep quality17.
The quality of life assessment
The 36-item Short-Form Health Survey was used to assess the quality of life. Each sub-score ranged from 0 to 100, with a higher score indicating a better quality of life18. The validity and reliability of this questionnaire in the Iranian population were 0.88 and 0.93, respectively, which is an acceptable coefficient19.
Anthropometric and body composition measurements
Weight and height were recorded in light clothing with no shoes using an OMRON digital scale and a plastic tape measure. The BMI and body composition indices (fat percentage, muscle mass, visceral fat) were measured and recorded by the OMRON (BF511) body composition analysis device in a 3-hour fasting state. Waist circumference was measured at the narrowest point between the lower rib and iliac crest at the end of normal expiration. Hip circumference was determined by measuring tape at the maximum point of gluteal muscles. Waist-to-hip ratio (WHR) was then calculated as waist divided by hip circumference.
Statistical analysis
The Kolmogorov-Smirnov test confirmed normal distributions of data. To analyze data, descriptive statistics including mean and standard deviation were used. Pearson correlation coefficient was used to show the relationship between variables at the significance level of p<0.05. Also, data were assessed using an independent t-test to determine if there were differences between groups. Data were analyzed using SPSS software 21 version.
RESULTS
Out of 392 students who participated in our study, 222 (56%) were female and 170 (44%) were male. The general indicators, body composition and demographic characteristics of the subjects by gender are presented in Table 1. The mean age of females and males was 24.7±3.8 years and 25.9±3.6 years, respectively. The mean value of subcutaneous fat in male and female students was higher than the normal range, but other body composition indices were normal in both sexes.
Table 1
Demographic characteristics and body composition measurements by gender
The mean values of drug use, quality of life, and sleep quality, are presented in Table 2. The use of alcohol, tobacco, cannabis, opioids and inhalants was significantly higher in males compared to females. There was a significant difference between males and females in terms of quality of life and sleep.
Table 2
Mean score of drugs consumption, quality of life and sleep quality stratified by gender
| Variables | Total(N=392) | Females (n=222) | Males (n=170) | p |
|---|---|---|---|---|
| Alcohol | 1.28±3.64 | 0.78±2.7 | 1.91±4.51 | 0.004** |
| Tobacco | 4.68±8.05 | 2.5±5.7 | 7.52±9.64 | 0.000** |
| Opioids | 0.62±2.75 | 0.36±2.07 | 0.95±3.42 | 0.045* |
| Cannabis | 0.44±2.3 | 0.16±1.37 | 0.80±3.08 | 0.012* |
| Amphetamine | 0.24±2.78 | 0.09±1.05 | 0.44±4.04 | 0.263 |
| Sedatives | 0.83±3.61 | 0.89±4.19 | 0.74±2.66 | 0.674 |
| Inhalants | 0.08±0.58 | 0.02±0.33 | 0.15±0.79 | 0.037* |
| Hallucinogens | 0.05±0.85 | 0.072±1.07 | 0.029±0.38 | 0.621 |
| Cocaine | 0.01±0.15 | 0 | 0.018±0.23 | 0.319 |
| Other drugs | 0.02±0.29 | 0 | 0.047±0.44 | 0.171 |
| Quality of life | 570.64±133.18 | 550.18±140.15 | 597.36±118.66 | 0.000** |
| Sleep quality | 5.44±3.32 | 5.73±3.58 | 5.06±2.9 | 0.042* |
As presented in Table 3, the most common substance use was tobacco with 33.67% (66% of males, 34% of females), alcohol 14.29% (66% of males, 34% of females), sedatives 8.16% (56% of males, 44% of females) and opioids 7.14% (71% of males, 29% of females). The usage rates of cannabis, inhalants, amphetamine, hallucinogens, unknown drugs and cocaine were about 4%, 2%, 1.53%, 0.51%, 0.51% and 0.26%, respectively.
Table 3
Frequency distribution of drug use by gender
In the present study, there was a significant and negative relationship between the level of quality of life and tobacco use (p<0.05) and sedatives (p<0.01), in dormitory students of Allameh Tabataba’i University. There was a significant and negative relationship between the subjects’ sleep quality and tobacco use (p<0.05), sedatives (p<0.01), inhalants (p<0.05), and other drugs (p<0.05). On the other hand, there was no significant relationship between the use of unknown drugs and students’ quality of life and sleep quality. The results of the Pearson correlation coefficient are presented in Table 4.
Table 4
Correlation between drug consumption and quality of life and sleep in students
| Variables | Quality of life | Quality of sleep | ||
|---|---|---|---|---|
| Sig | Pearson | Sig | Pearson | |
| Alcohol | 0.548 | -0.03 | 0.16 | 0.071 |
| Tobacco | 0.037* | -0.106 | 0.011* | 0.12 |
| Opioids | 0.778 | -0.014 | 0.891 | -0.007 |
| Cannabis | 0.662 | 0.025 | 0.591 | 0.027 |
| Amphetamine | 0.128 | -0.077 | 0.825 | 0.011 |
| Sedatives | 0.004** | -0.145 | 0.001** | 0.173 |
| Inhalants | 0.564 | 0.029 | 0.048* | 0.1 |
| Hallucinogens | 0.708 | -0.019 | 0.783 | -0.014 |
| Cocaine | 0.177 | 0.068 | 0.299 | -0.053 |
| Other drugs | 0.458 | 0.038 | 0.028* | 0.111 |
| Age | 0.93 | 0.004 | 0.449 | -0.038 |
| BMI | 0.299 | -0.053 | 0.213 | 0.063 |
| WHR | 0.756 | 0.016 | 0.671 | -0.022 |
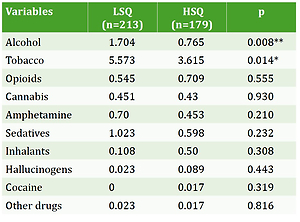
We divided the subjects into two groups both for sleep quality and quality of life using an independent t-test. Compared with the low sleep quality (LSQ) group, the high sleep quality (HSQ) group showed significantly lower alcohol and tobacco consumption (Table 5). On the other hand, the use of sedatives in the group with poor quality of life was significantly higher than the group with a high quality of life (Table 6).
Table 5
Comparison of drug use in subjects with low and high sleep quality
| Variables | LSQ (n=213) | HSQ (n=179) | p |
|---|---|---|---|
| Alcohol | 1.704 | 0.765 | 0.008** |
| Tobacco | 5.573 | 3.615 | 0.014* |
| Opioids | 0.545 | 0.709 | 0.555 |
| Cannabis | 0.451 | 0.43 | 0.930 |
| Amphetamine | 0.70 | 0.453 | 0.210 |
| Sedatives | 1.023 | 0.598 | 0.232 |
| Inhalants | 0.108 | 0.50 | 0.308 |
| Hallucinogens | 0.023 | 0.089 | 0.443 |
| Cocaine | 0 | 0.017 | 0.319 |
| Other drugs | 0.023 | 0.017 | 0.816 |
Table 6
Comparison of drug use among subjects with high (QoL ≥570.6) and poor (QoL <570.6) quality of life
| Variables | High QoL (n=220) | Poor QoL (n=172) | p |
|---|---|---|---|
| Alcohol | 1.118 | 1.477 | 0.334 |
| Tobacco | 4.077 | 5.448 | 0.103 |
| Opioids | 0.682 | 0.541 | 0.615 |
| Cannabis | 0.445 | 0.436 | 0.968 |
| Amphetamine | 0.023 | 0.529 | 0.114 |
| Sedatives | 0.473 | 1.285 | 0.039* |
| Inhalants | 0.095 | 0.064 | 0.597 |
| Hallucinogens | 0.073 | 0.029 | 0.613 |
| Cocaine | 0.014 | 0 | 0.377 |
| Other drugs | 0.036 | 0 | 0.171 |
DISCUSSION
The high prevalence of drug use, especially among students, has detrimental effects on different organs of the body and can change the students’ normal life path. The effects of drugs on people’s lives can be examined in different ways. It can be noted that the relationship between drug use and students’ sleep quality and quality of life in dormitories has been little examined. Lack of research in this area can lead to circumstances that endanger the health of these students and to a decrease in the level of health in the community.
In the present study, the rate of alcohol consumption among students was 14.03%, its prevalence was significantly higher in male students. Alcohol consumption was significantly higher in the LSQ group compared to the HSQ group. Alcohol consumption leads to a presynaptic release of GABA in the brain stem and spinal cord and increases the function of GABA receptors in other brain regions such as the thalamus and cortex, associated with reduced stimulation threshold of calcium channels. As a result, with increased activity of neurotransmitters in the brain, the excitation mechanisms of cholinergic and noradrenergic in the brain stem are increased compared to individuals who have not consumed alcohol, leading to an increase in sleep disturbances and a decrease in sleep quality of individuals who consume alcohol20.
A significant and negative relationship was noted between tobacco consumption and sleep quality of dormitory students. Tobacco smoking was significantly higher in the poor sleep quality group compared with the good sleep quality group. Dugas et al.21 in a study of 1294 adolescent students aged 24 years, recruited in 2000–2011, observed a significant and negative correlation between nicotine consumption and sleep quality. The main ingredient of tobacco is nicotine, which is highly addictive and has devastating effects on various body systems including cardiovascular, reproductive, urinary, and respiratory diseases22. There is a mechanism by which tobacco consumption affects sleep quality; this effect happens immediately after the consumption, when the blood nicotine level increases and it is associated with an increase in heart rate, blood pressure, faster breathing and an increase in catecholamine secretion from the central cortex of the adrenal glands23. The increased release of norepinephrine and dopamine, stimulates adrenergic neurons in the brain, which increases the level of consciousness24 and consequently lowers the quality of sleep in individuals. In addition, nicotine consumption leads to suprachiasmatic nucleus (SCN) damage in the hypothalamus and disrupts the rhythm of sleep and awakening, and accordingly impacts negatively on students’ sleep quality25.
In the present study, there was a significant and negative relationship between sedative substances and sleep quality in dormitory students. Students tend to consume sedative medications for several reasons such as suffering different stress, dormitory unfavorable situations, and exams anxiety. The studies of Karami et al.26 reported that the use of sedative medications improves sleep quality. The reason of the contradiction between our findings with previous studies is the difference in the time of consumption by students; the lack of full absorption and most importantly irregular consumption and a low dose of substances in dormitory students are among the reasons.
We identified a significant and negative relationship between the use of an inhalant substance and sleep quality in students. Our findings are in line with the research carried out by Patra et al.27. Inhalation products include solvents (fluids that convert to gas at room temperature), aerosol sprays, gases, and nitrites. Most people do not have complete information on this matter, and they are not familiar with these substances as addictive drugs, while such substances can have serious health consequences. The use of these substances increases heart rate and reduces oxygen supply to tissues28. In the present study, there was a significant and negative relationship between the use of other drugs and the quality of sleep in students. It is impossible to provide accurate information, due to an inability to identify exact substances and also because of low consumption of these substances; but it can be argued that the use of these unknown drugs, which are sometimes considered as less harmful and addictive substances, is associated with poor sleep quality and could have irreversible consequences in the long-term.
We also noted a significant and negative relationship between tobacco consumption and quality of life in students. Our findings are supported by a previous study13. Besides the mentioned physiological effects of nicotine consumption, it affects psychosocial, social and health aspects of people, significantly reducing quality of life. Talati et al.29 in 2016 reported that nicotine consumption increases anxiety and depression in individuals and also reduces quality of life, while its consumption is considered as a sedative factor in the public’s view. There was a significant and negative relationship between the use of sedative substances and the students’ quality of life. Also, sedatives use in the high QoL group was significantly lower than the poor QoL group. Sedative drugs reduce the activity of neurotransmitter receptors and lead to an individuals’ mental and physical calmness30, and so improve the mental quality of life; however, our findings indicate that there is a negative correlation between sedative drugs and the students’ quality of life. Since the overall score of quality of life was calculated in this study, the use of these substances may have only a positive impact on the mental scale with adverse effects seen in other dimensions.
Strengths and limitations
Some limitations of this study should be mentioned, such as the small sample; if more universities were recruited from Tehran and other cities, more accurate information about the prevalence of drug use among students in different cities and other parts of Tehran could be achieved. Also, using anxiety, stress and life expectancy questionnaires could be effective in identifying the causes and the relationship between these factors and drug use in students. Strengths of this study include the fact that unlike most previous studies conducted in Iran, our study used the ASSIST questionnaire to fully examined various drugs. Also, we examined drug use in both genders, which let us compare drug consumption between females and males.
CONCLUSIONS
According to the findings of this study, it can be stated that drug consumption among students besides having destructive effects on physiological systems of the body, leads to dysfunction in sleep quality and a decrease in quality of life.